Better care between visits. Better revenue from day one.
CareAtlas embeds dedicated care navigators and clinicians — real people, supported by AI — into your organization to manage RPM, CCM, TCM, and APCM programs. No upfront investment required for hospitals. Practices see revenue from month one. Patients stay healthier at home.
23%
reduction in 30-day readmissions
4+
navigator touches per patient per month
30+
vital readings per patient per month
HIMSS26
Emerge Experience Winner's Circle — Hospital Systems category


Real people. Real relationships. Real results.
Healthcare doesn't need more technology — it needs more people, supported by technology. Our care navigators build genuine relationships with your patients, licensed clinicians oversee every care plan, and AI handles the complexity behind the scenes.

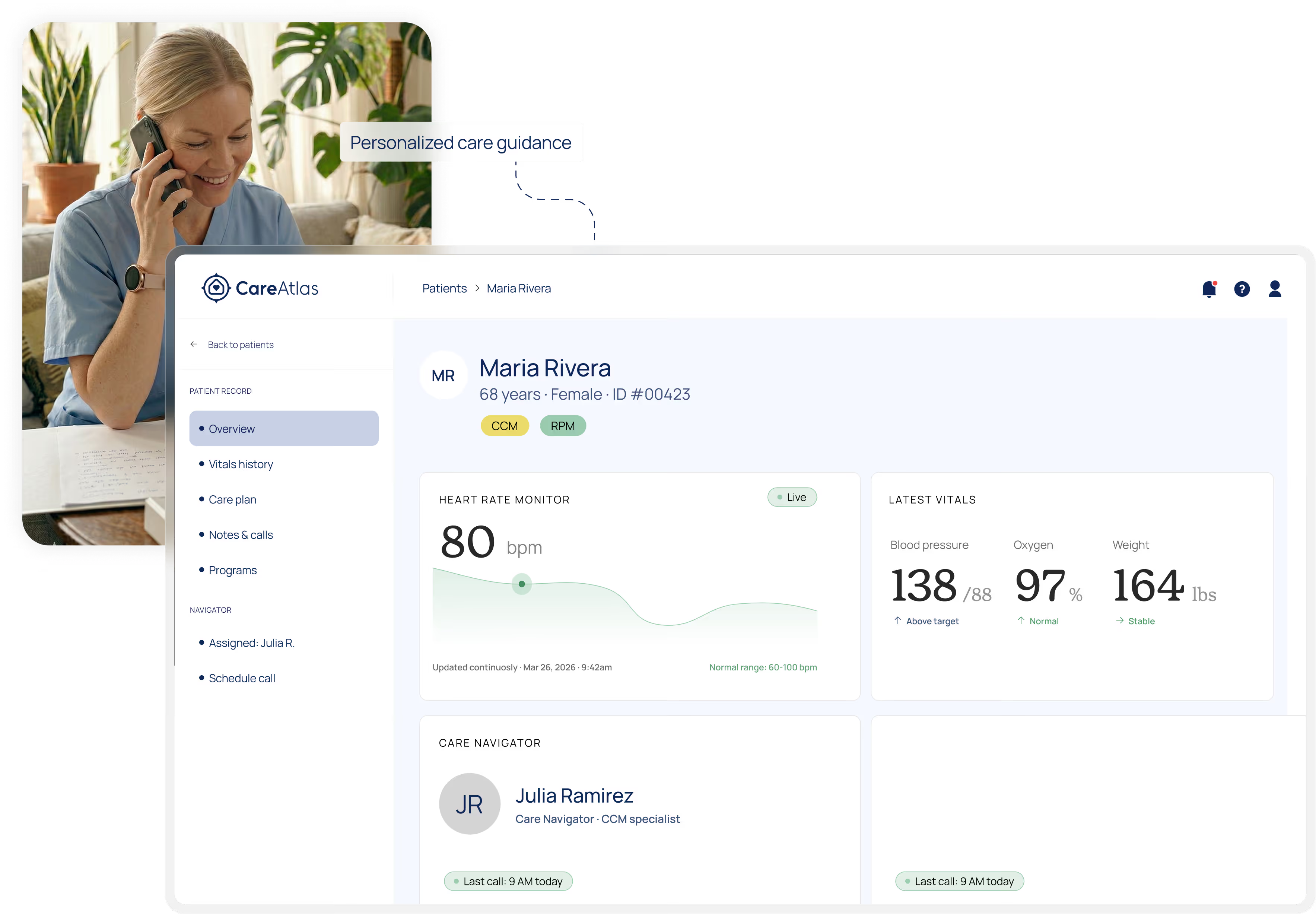
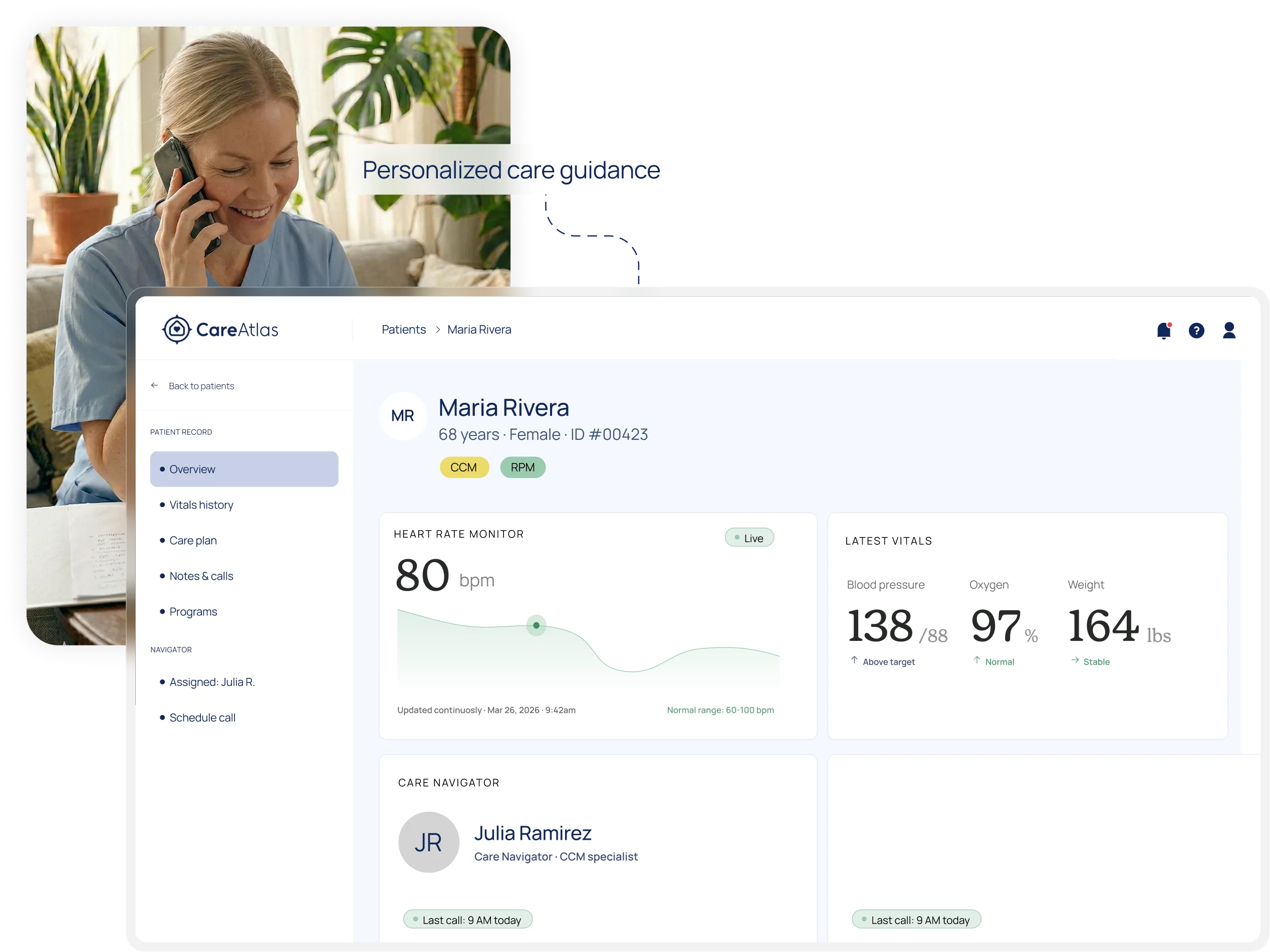
A named navigator for every patient
Your patients get a dedicated care navigator who knows their name, calls them regularly, and helps them manage their conditions. Not a chatbot. Not an app. A person.

AI that works for your team,
not instead of it
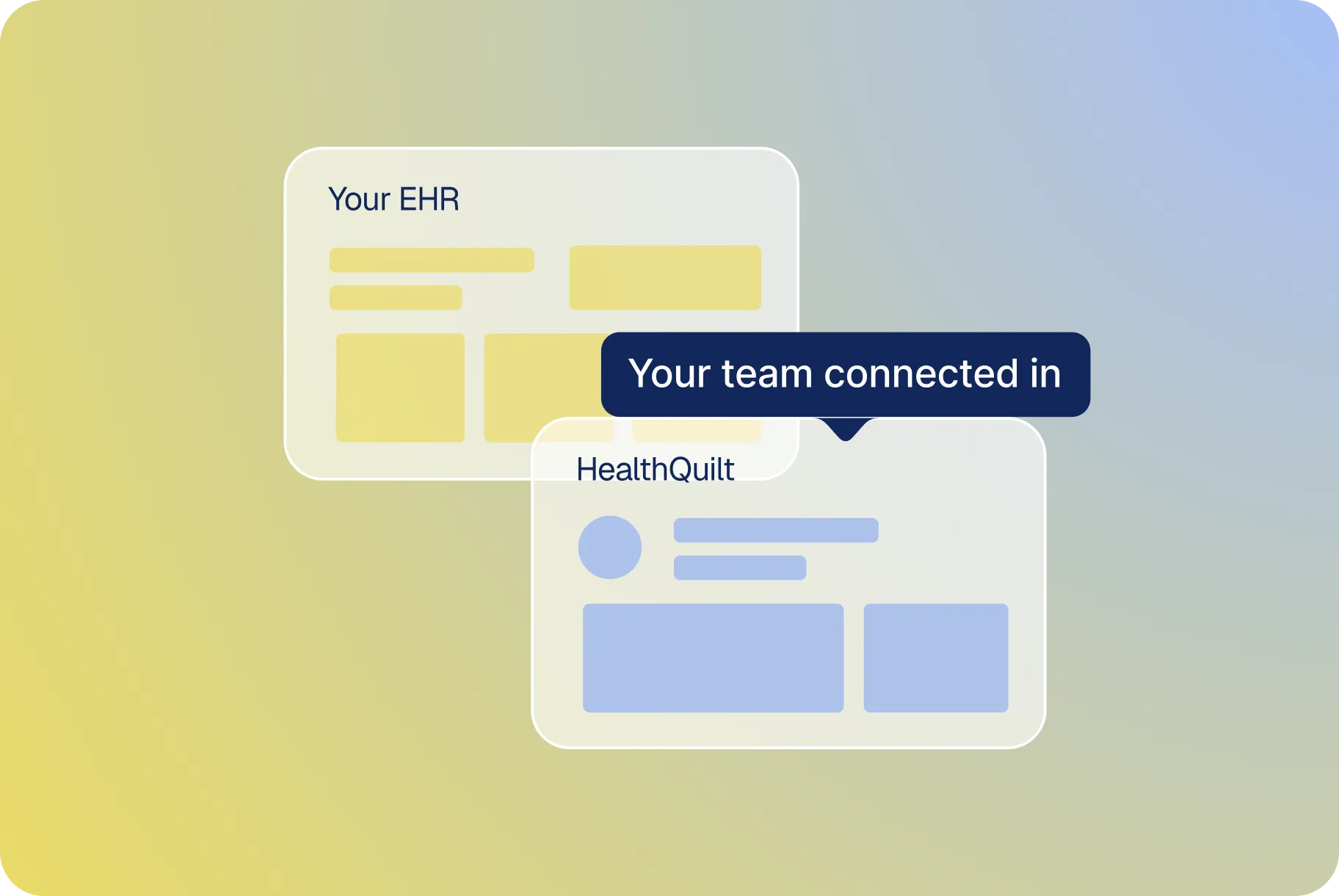
HealthQuilt, our proprietary platform, automates documentation, surfaces care gaps, and prioritizes high-risk patients — so navigators spend their time on what matters: patient relationships.

Outcomes that hold up to scrutiny
14.8% readmission rate vs. the 19% CMS benchmark — a 23% relative reduction in a high-risk Medicare population (89% age 65+, 38% COPD, 24% CHF). 73% device adherence. About 85% six-month retention. Results from a 145-patient RPM/CCM cohort, October 2025.
One partner. Four programs. Minimal burden on your team.
CareAtlas manages the full spectrum of Medicare care coordination — RPM, CCM, TCM, and APCM — end to end. We handle enrollment, care delivery, documentation, and billing. Your staff stays focused on what they do best.

Refer
Hospital or clinic refers eligible patients

Enroll
CareAtlas navigators onboard patients with senior-friendly devices (no WiFi needed)

Monitor & Engage
Daily monitoring, regular navigator check-ins, AI-assisted care plans

Document & Bill
Automated compliance documentation and Medicare billing

Report
Clinical insights flow back to the PCP inside their existing EHR
CareAtlas Complete
Full-service care coordination. We provide the navigators, technology, devices, enrollment, billing, and care delivery — end to end. For hospitals, CareAtlas serves as provider of record — no upfront investment required. For practices and community health centers, revenue consistently exceeds program costs.
CareAtlas Extend
Already have some care coordination staff? We augment your team with the HealthQuilt platform, device logistics, and overflow navigator support — filling gaps without replacing what works.
CareAtlas Connect
Platform-only access to HealthQuilt — our AI-assisted care coordination software, EHR integration, analytics, and compliance tools. You bring the team. We bring the technology.


Designed for how healthcare actually works.
Whether you're a community hospital, a multi-site physician network, an FQHC, or a value-based organization — CareAtlas is built for the realities of your practice, not retrofitted from an enterprise product.

Hospital + Health Systems
CareAtlas serves as provider of record through our affiliated professional corporation — a partnership with no upfront investment required, no new hires required. We manage RPM, CCM, TCM, and APCM across service lines, reduce readmissions, and capture the Medicare reimbursement these programs generate. Proven in community and rural settings.

Physician Practices
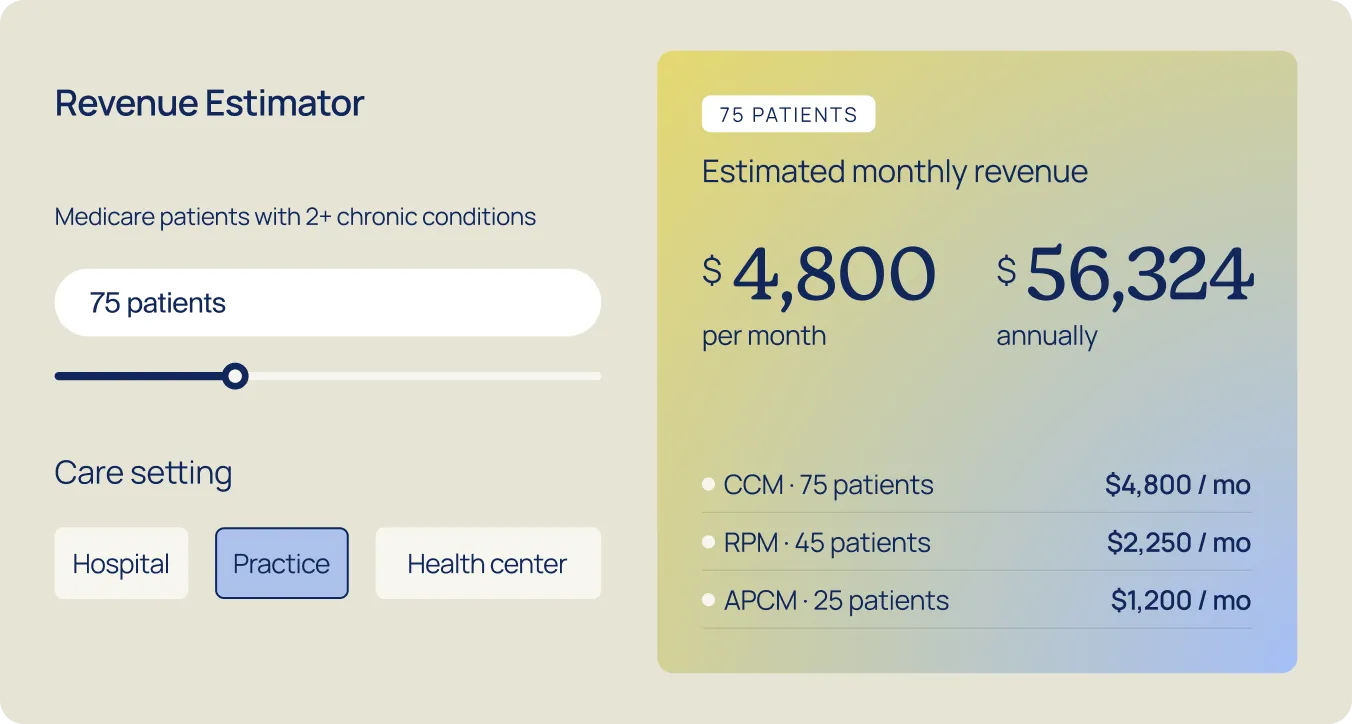
Generate $50–$120 per patient per month in new Medicare revenue without adding staff or complexity. We handle enrollment, monitoring, documentation, and billing. You keep the patient relationship and stay provider of record.
Revenue varies by program mix, volume, and payer. Not a guarantee of income.


Four programs. One partner. Every eligible dollar captured.
Most organizations cobble together multiple vendors for RPM, CCM, TCM, and APCM — or leave the revenue on the table entirely. CareAtlas manages all four under one roof, maximizing reimbursement per patient.
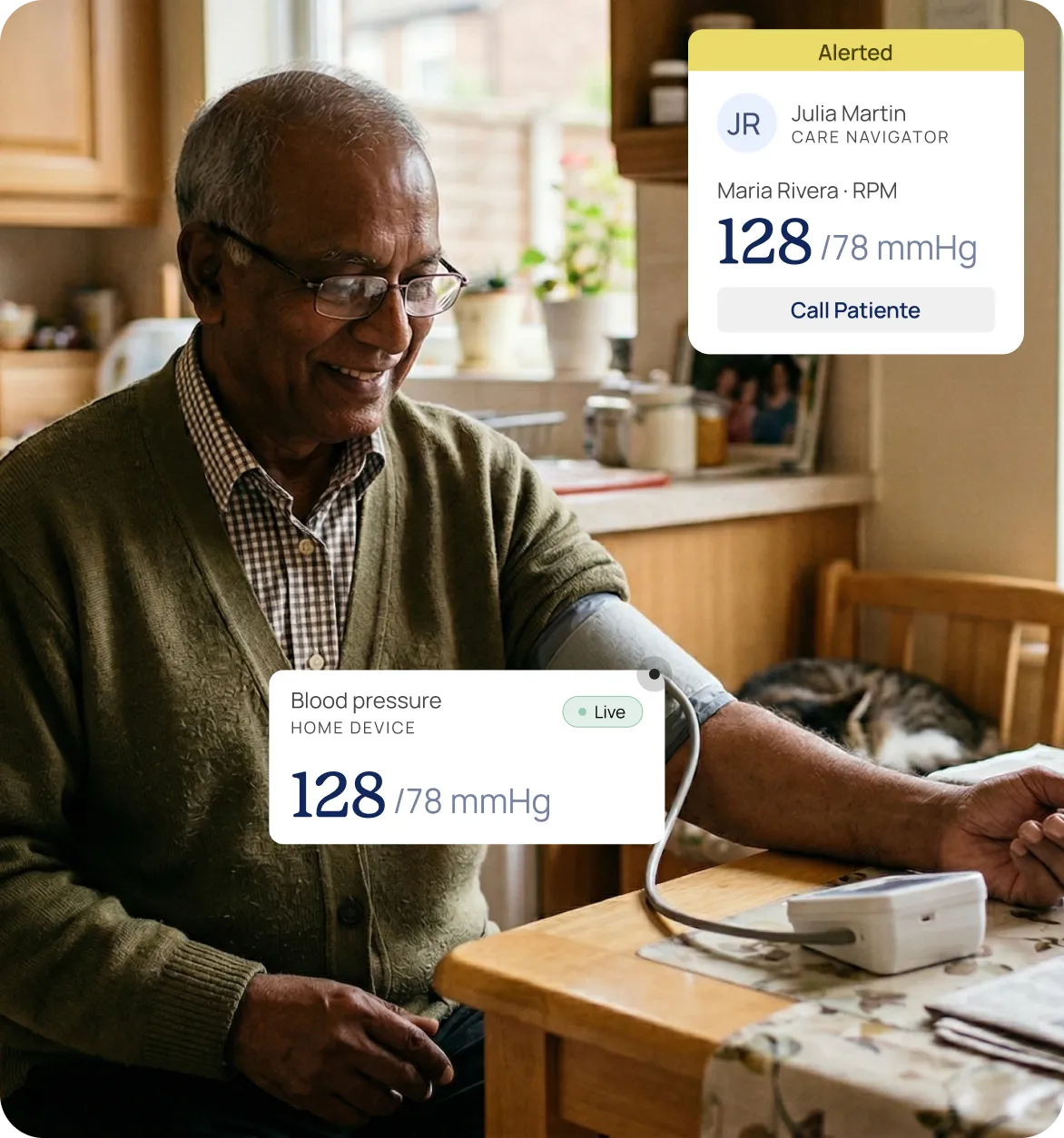
Remote Patient Monitoring
RPM: Daily visibility into patient health
Cellular-connected devices ship directly to patients — blood pressure cuffs, glucose monitors, pulse oximeters, scales. No WiFi. No smartphone. No patient app. Daily readings are monitored by dedicated care navigators with AI-assisted alerts that catch deterioration before it becomes an ER visit.
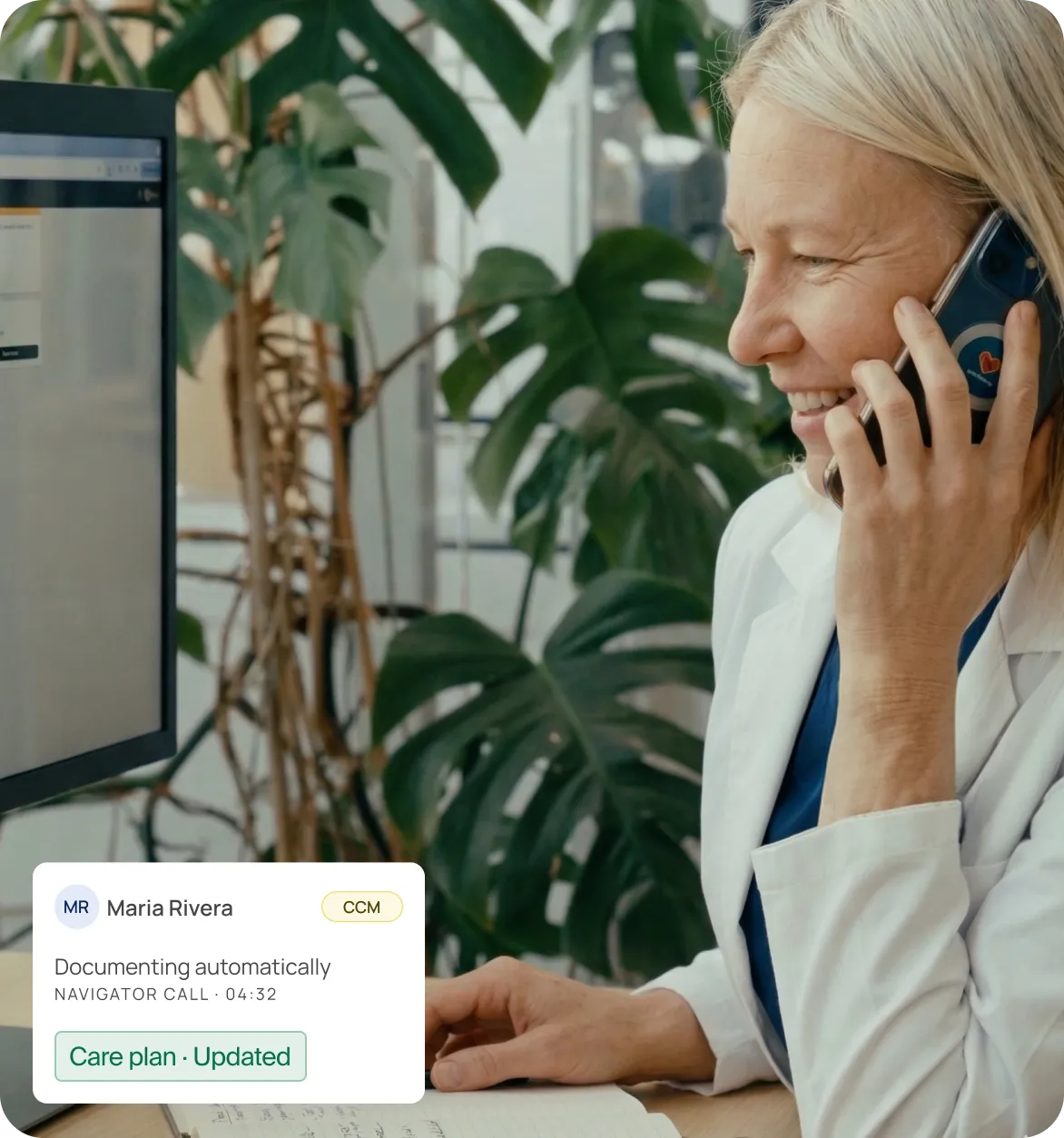
Chronic Care Management
CCM: Consistent care between appointments
Monthly navigator check-ins, personalized care plans, medication management, and social determinant screening — all documented and billed under 99490/99491. Only about 18% of eligible Medicare discharges receive a TCM bill, even though roughly 52% of unbilled eligible discharges already had a qualifying visit within 14 days. CareAtlas helps close that gap.
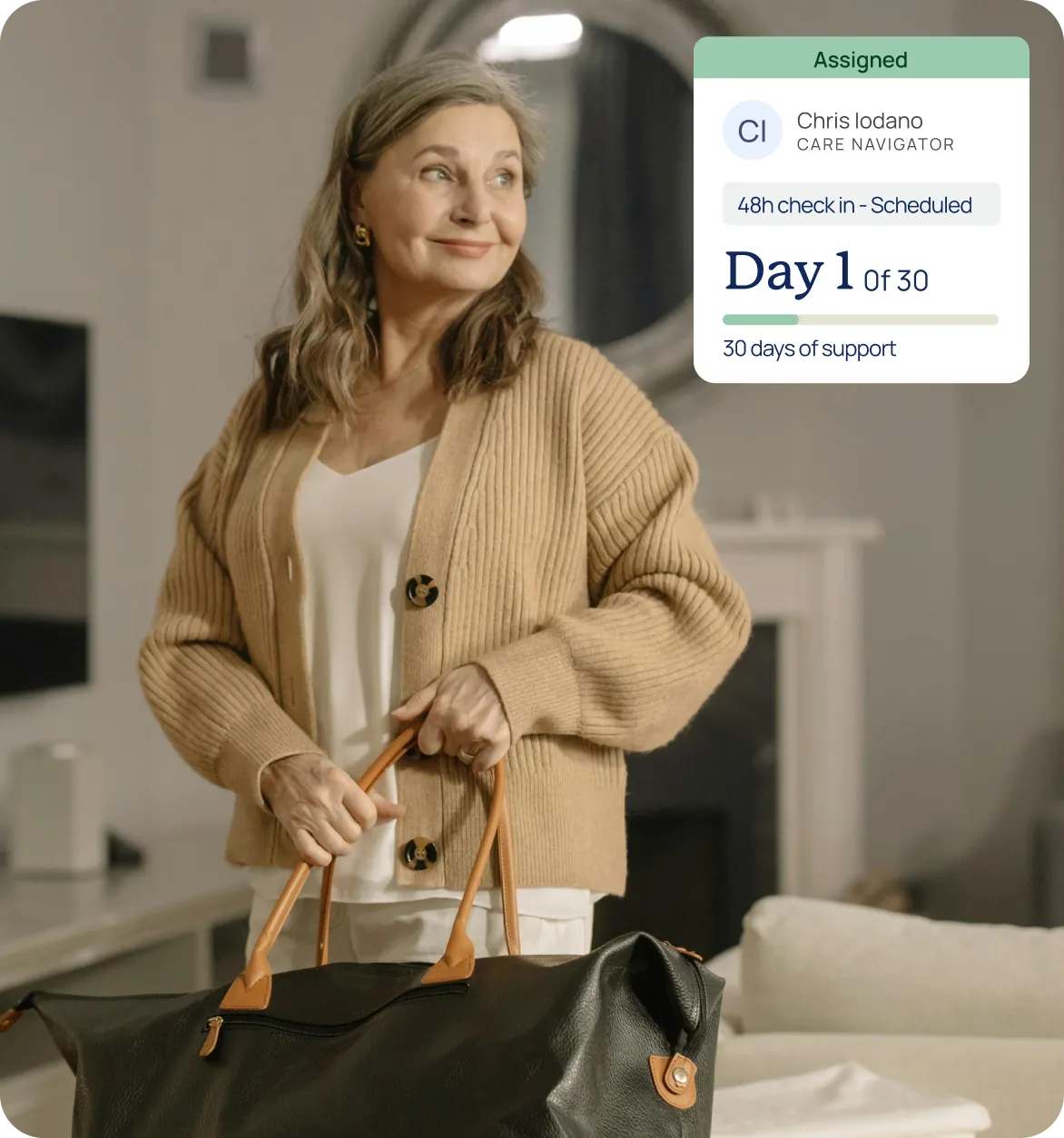
Transitional Care Management
TCM: The critical 30 days after discharge
Navigator outreach within 48 hours of discharge. Medication reconciliation. Follow-up scheduling. 30 days of transition support during the window when patients are most vulnerable — and when the vast majority of billable TCM episodes go uncaptured. Only about 18% of eligible Medicare discharges are billed for TCM (HHS ASPE/NORC, 2019 claims), and among those unbilled, over half already had a qualifying office visit within 14 days — revenue left on the table.
Advanced Primary Care Management
APCM: The newest Medicare revenue pathway
APCM reimburses across three risk-stratified tiers — $16/mo (Level 1), $54/mo (Level 2), and $117/mo (Level 3) — with no time-tracking requirements. For a panel of 200 patients at Level 2, that's ~$129K/year in recurring revenue, billable alongside RPM.


"CareAtlas is superior to what I currently use, our existing platform is just a timer and a billing module. CareAtlas really integrates into my workflow, brings in relevant data and meaningfully suggests insights.”
Physician, Texas-based Health System.

